

Fowl cholera is one of the most serious bacterial diseases in poultry farming. It is highly contagious, can affect a wide range of avian species including chickens, turkeys, and waterfowl, and in its most severe form can kill up to 100% of an affected flock. Understanding how it spreads, what it looks like, and how to respond is essential for any poultry farmer who wants to protect their birds and their business.
The disease is caused by the bacterium Pasteurella multocida and enters birds through the oral or nasal route. Transmission occurs through nasal discharge, droppings, contaminated soil, equipment, and people moving between flocks. The incubation period is typically 5 to 8 days. While the bacterium is easily destroyed by disinfectants, sunlight, heat, and drying, it can persist in soil for extended periods, making thorough environmental management critical after an outbreak.
1. Fowl Cholera Etiology and Transmission
Pasteurella multocida is a small, gram-negative, non-motile rod-shaped bacterium with a capsule. It is classified as a single species but includes three subspecies: multocida, septica, and gallicida. Subspecies multocida is the most common cause of disease, though the other two can also cause cholera-like illness in birds.
Although P. multocida infects a wide variety of animals, strains isolated from non-avian hosts generally do not produce fowl cholera. The strains that do cause the disease exist in multiple serotypes, which makes developing a universally effective vaccine challenging.
A. Susceptibility
Not all birds are equally at risk. Turkeys and waterfowl are more susceptible than chickens. Among chickens, older birds are more vulnerable than young ones, and some breeds are more susceptible than others. High stocking density and concurrent infections, particularly respiratory viruses, are predisposing factors that increase the likelihood and severity of an outbreak.
B. Sources of Infection
Chronically infected birds and birds that carry the organism without showing symptoms are the primary sources of infection within and between flocks. Wild birds can introduce the organism into a flock. Rodents, pigs, dogs, and cats can also carry P. multocida, though the exact role of these mammals as long-term reservoirs has not been fully established.
Within a flock, the disease spreads primarily through secretions from the mouth, nose, and eyes of infected birds that contaminate the surrounding environment. P. multocida can also survive long enough on contaminated crates, feed bags, footwear, and equipment to be carried between houses. The infection is not transmitted through eggs.
2. Clinical Findings

Clinical signs vary significantly depending on the form of the disease.
A. Acute Fowl Cholera
In acute cases, the first sign is often finding a large number of dead birds with no obvious prior warning. Mortality rises rapidly once it begins. In less sudden presentations, affected birds show depression, loss of appetite, mucoid discharge from the mouth, ruffled feathers, diarrhea, and increased respiratory rate. Pneumonia is particularly common in turkeys.
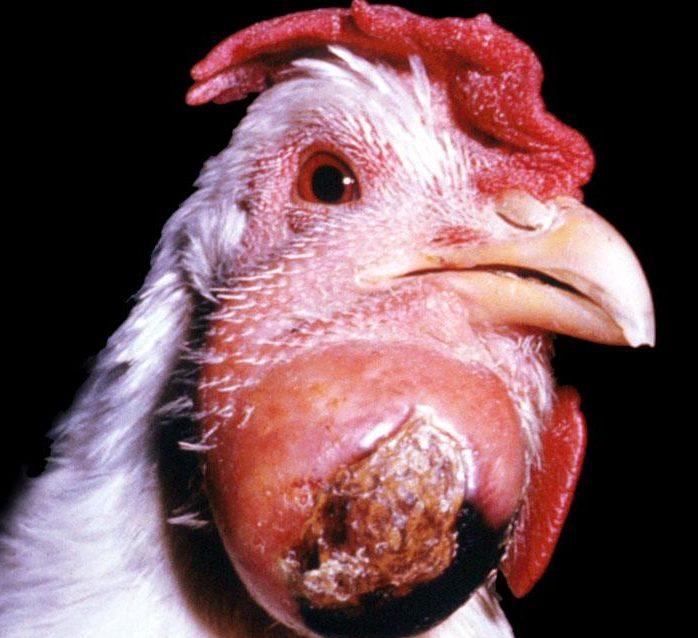
B. Chronic Fowl Cholera
In the chronic form, signs are generally related to localized infections. Swelling of the sternal bursae, wattles, joints, tendon sheaths, and footpads is common, caused by accumulated fibrinosuppurative material. Exudative conjunctivitis and pharyngitis may also occur. When the meninges, middle ear, or cranial bones become infected, birds may develop torticollis, an abnormal twisting of the neck.
Read Also: Importance of Multivitamins in Poultry Production
3. Fowl Cholera Lesions

Post-mortem findings reflect the severity and stage of infection.
In peracute and acute cases, lesions are primarily vascular. General congestion and passive hyperemia are visible throughout the carcass, accompanied by enlargement of the liver and spleen. Petechial and ecchymotic hemorrhages are common, particularly in subepicardial and subserical locations. Increased amounts of peritoneal and pericardial fluid are frequently present. In laying birds, acute oophoritis with hyperemic follicles may be seen. In subacute cases, multiple small necrotic foci are scattered throughout the liver and spleen.
In chronic infections, suppurative lesions are more widely distributed and often involve the respiratory tract, the conjunctiva, and the tissues surrounding the head. Caseous arthritis and productive inflammation of the peritoneal cavity and oviduct are common findings. In turkeys and broilers, a fibrino-necrotic dermatitis affecting the back, abdomen, and breast, involving the skin, subcutaneous tissue, and underlying muscle, has been documented. Necrotic lung lesions should always raise suspicion of fowl cholera.
4. Fowl Cholera Diagnosis

History, clinical signs, and post-mortem findings can point strongly toward fowl cholera, but confirmation requires laboratory isolation and identification of P. multocida. Primary isolation is performed using blood agar, dextrose starch agar, or trypticase soy agar. Adding 5% heat-inactivated serum to the media improves isolation success.
P. multocida can be readily isolated from the organs of birds dying from acute fowl cholera. Isolation from suppurative lesions in chronic cases can be more difficult. At post-mortem examination, staining of smears from the liver is useful in acute cases. Immunofluorescent microscopy and in situ hybridization have also been used to identify the organism in infected tissues.
Polymerase Chain Reaction (PCR) testing can detect P. multocida in pure and mixed cultures and clinical samples and may help identify carrier animals within flocks. Serological testing options include rapid whole blood agglutination, serum plate agglutination, agar diffusion, and ELISA, though serology has limited diagnostic value and is used mainly to evaluate vaccine responses.
Several other bacterial infections can produce lesions that are visually indistinguishable from fowl cholera on post-mortem examination alone. These include Escherichia coli, Salmonella enterica, Ornithobacterium rhinotracheale, gram-positive cocci, and Erysipelothrix rhusiopathiae. Laboratory confirmation is therefore essential before concluding a diagnosis.
5. Fowl Cholera Prevention

Prevention starts with strong biosecurity and sound management practices. Rodents, wild birds, pets, and other animals that may carry P. multocida must be kept out of poultry houses at all times.
Vaccination plays an important role in areas where the disease is prevalent. Adjuvant bacterins are widely used and generally effective. When polyvalent bacterins prove ineffective, autogenous bacterins made from strains isolated from the affected flock are recommended. Knowing the predominant local serotypes is important for selecting the right vaccine product.
Attenuated live vaccines are also available. These are administered in drinking water for turkeys and by wing-web inoculation for chickens, and they can stimulate immunity against multiple serotypes of P. multocida. Live vaccines should only be used in healthy flocks.
Read Also: Bird flu in the Poultry Farm and How to tackle it
6. Fowl Cholera Treatment

Treatment can lower mortality during an active outbreak, but it is important to understand that drugs do not eliminate P. multocida from the flock. When treatment stops, deaths often resume. True eradication of the infection requires complete depopulation, followed by thorough cleaning and disinfection of all buildings and equipment, and then keeping the premises free of birds for several weeks.
Sulfonamides and antibiotics are the standard treatment options. Early intervention and adequate dosing are critical. Sensitivity testing is strongly recommended because multi-resistant strains have emerged in many areas. Sulfaquinoxaline sodium in feed or water typically controls mortality effectively, as do sulfamethazine and sulfadimethoxine. Sulfonamides should be used with caution in breeding birds due to potential toxicity.
Tetracycline antibiotics at high levels, either in feed, drinking water, or administered parenterally, can also be effective. Norfloxacin via drinking water has shown efficacy against fowl cholera, though many countries prohibit the use of quinolones in food-producing animals due to concerns about antimicrobial resistance development. Penicillin is often effective for sulfa-resistant infections. In ducks, a combined injection of streptomycin and dihydrostreptomycin has proven useful.
All treatment decisions should be made in consultation with a qualified veterinarian who can guide drug selection, dosing, and withdrawal periods.
Summary on Fowl Cholera Disease: Causes, Signs, Diagnosis, and Treatment
| Topic | Key Points |
|---|---|
| Cause | Pasteurella multocida, a gram-negative bacterium. Subspecies multocida is most common. |
| Transmission | Oral or nasal route. Spread through secretions, droppings, contaminated equipment, and carrier animals. Not egg-transmitted. |
| Incubation Period | 5 to 8 days. |
| Most Susceptible Birds | Turkeys and waterfowl more than chickens. Older birds more than young birds. |
| Acute Signs | Sudden death, depression, anorexia, mucoid oral discharge, ruffled feathers, diarrhea, increased respiratory rate. |
| Chronic Signs | Swollen wattles, joints, and footpads. Conjunctivitis, pharyngitis, torticollis in severe cases. |
| Key Lesions | Congestion, hemorrhages, enlarged liver and spleen, necrotic foci, caseous arthritis in chronic cases. |
| Diagnosis | Laboratory isolation of P. multocida required for confirmation. PCR, smear staining, and serology also used. |
| Prevention | Strict biosecurity, exclusion of carrier animals, vaccination with bacterins or live attenuated vaccines. |
| Treatment | Sulfonamides, tetracyclines, penicillin, or norfloxacin under veterinary guidance. Treatment reduces mortality but does not eliminate the organism. Eradication requires depopulation and full disinfection. |
Frequently Asked Questions About Fowl Cholera Disease
1. What causes fowl cholera and how serious is it?
Fowl cholera is caused by the bacterium Pasteurella multocida. It is one of the most serious bacterial diseases in poultry because it spreads rapidly and can kill up to 100% of an affected flock in its most severe acute form. It affects chickens, turkeys, waterfowl, and other avian species, and can range from sudden mass death to chronic localized infections that persist in a flock over a long period.
2. How does fowl cholera spread between and within flocks?
The disease spreads primarily through secretions from the mouth, nose, and eyes of infected birds that contaminate the environment, feed, and water. It can also be carried on contaminated equipment, crates, feed bags, and footwear. Wild birds, rodents, cats, pigs, and dogs can serve as carriers. The infection is not transmitted through eggs.
3. Which birds are most at risk of fowl cholera?
Turkeys and waterfowl are more susceptible than chickens. Among chickens, older birds are more vulnerable than younger ones. Some chicken breeds also show higher susceptibility than others. High stocking density and concurrent respiratory infections are additional risk factors that increase both the likelihood of an outbreak and its severity.
4. What are the first signs of fowl cholera in a flock?
In acute cases, the first sign is often finding multiple dead birds without any prior warning. Mortality then rises rapidly. In less sudden outbreaks, signs include sudden depression, reduced feed intake, mucoid discharge from the mouth, ruffled feathers, watery diarrhea, and labored breathing. Pneumonia is a particularly common finding in turkeys.
5. How is fowl cholera diagnosed accurately?
A definitive diagnosis requires laboratory isolation and identification of Pasteurella multocida from affected birds. Blood agar and similar culture media are used for isolation. PCR testing can also detect the organism in clinical samples and is useful for identifying carrier birds. Post-mortem smear staining from the liver is helpful in acute cases. Several other bacterial infections produce similar-looking lesions, so laboratory confirmation is essential before concluding a diagnosis.
6. Can fowl cholera be fully eliminated from a flock with treatment?
No. Drug treatment reduces mortality during an active outbreak but does not eliminate P. multocida from the flock. Once treatment stops, the disease often returns. True eradication requires complete depopulation of the affected site, followed by thorough cleaning and disinfection of all buildings and equipment, and keeping the premises free of birds for several weeks before restocking.
7. What drugs are used to treat fowl cholera?
Sulfonamides are the most commonly used treatment and include sulfaquinoxaline sodium, sulfamethazine, and sulfadimethoxine. Tetracycline antibiotics at high levels are also effective. Penicillin works well for sulfa-resistant strains. Norfloxacin is effective but is prohibited in food-producing animals in many countries. Sensitivity testing before treatment is strongly recommended because multi-resistant strains have become common. All treatment should be done under veterinary supervision.
8. How can fowl cholera be prevented on a poultry farm?
Prevention relies on strict biosecurity. This means keeping wild birds, rodents, cats, and other potential carriers out of poultry houses, controlling access to the farm, and maintaining thorough hygiene practices. Vaccination is also important in areas where the disease is prevalent. Both bacterin vaccines and attenuated live vaccines are available. Knowing the predominant local serotypes helps ensure the right vaccine is selected.
9. Are there any restrictions on the antibiotics used to treat fowl cholera?
Yes. Quinolones such as norfloxacin are restricted or banned for use in food-producing animals in many countries due to the risk of antimicrobial resistance developing in strains that could affect human health. Always check current regulations in your country before selecting a treatment drug, and only use antibiotics under veterinary prescription and guidance with strict attention to withdrawal periods before slaughter.
10. Can carrier birds spread fowl cholera without showing symptoms?
Yes. Asymptomatic carrier birds are considered one of the primary sources of infection within flocks and between farms. These birds harbor P. multocida without showing visible signs of disease but shed the organism in their secretions. This is one of the reasons why PCR testing is valuable for flock health monitoring and why strict biosecurity, including quarantine of new birds before introduction, is essential for preventing the disease from entering a clean flock.
Do you have any questions, suggestions, or contributions? If so, please feel free to use the comment box below to share your thoughts. We also encourage you to kindly share this information with others who might benefit from it. Since we can’t reach everyone at once, we truly appreciate your help in spreading the word. Thank you very much for your support and for sharing!
Read Also: Feed and Nutrition Management for Cattle